
General Principles
Atraumatic Shoulder Pain
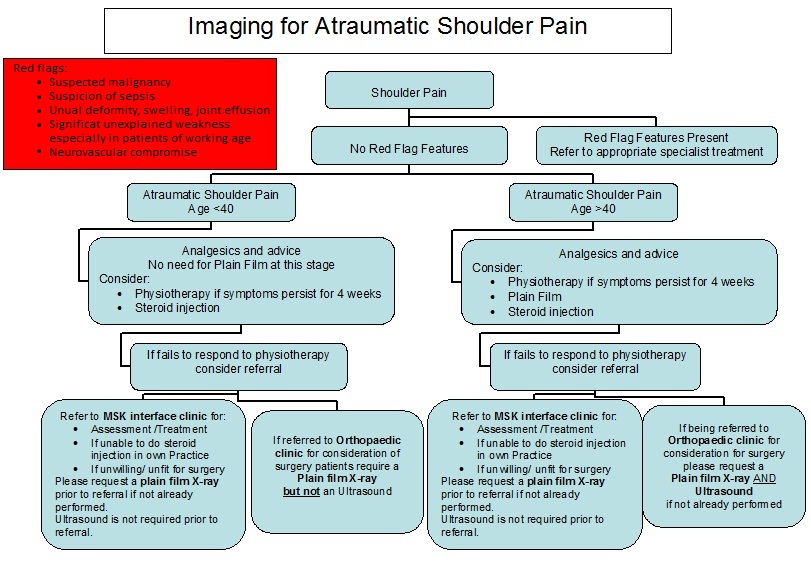
Common diagnoses:
- Impingement
- Rotator cuff tear
- Frozen shoulder
- Osteoarthritis acromio-clavicular joint
- Osteoarthritis of gleno-humeral joint
- Instability
Initial management is similar in the absence of red flags:
- Analgesics +/- physiotherapy: Note the exception of acute cuff tears above
Further management if symptoms persist beyond 4 weeks:
- Physiotherapy if not yet initiated
- Plain X-ray in patients aged under 20 or over 40 years
If failing to respond to physiotherapy:
-
Steroid injection
- Sub-acromial for impingement,
- Gleno-humeral for frozen shoulder and early/moderate OA
- Acromio-clavicular joint for ACJ pain
- Plain film if not already obtained
-
Referral to:
-
- Assessment & treatment
- Steroid injection
-
Orthopaedics for opinion / consideration for surgery
- Plain film required to exclude significant sub-acromial spurring, calcific tendonitis, ACJ or glenohumeral OA
-
General referral criteria for surgery (excluding conditions requiring immediate referral):
- State if any trauma or not
- Symptoms for at least 3 months if atraumatic
- Symptoms causing functional or social impairment
- Symptoms of instability
- No response to conservative measures: please detail what, in particular current analgesia
- If previous injections please state site
- Patient willing to undergo surgery
- Patient is fit for surgery
Imaging required prior to Orthopaedic referral:
-
X-ray
- Indicated in all patients with restricted active and passive range of movement to exclude OA
- True AP X-ray and Axillary view (if patient cannot abduct arm to nearly 90 degrees a trauma axillary view may be done instead)
- In patients over 40 yrs with persistent impingement pain, plain films may help identify sub-acromial spurring, AC joint OA or calcific tendonitis
- USS – Should be considered prior to surgical referral in Patients > 40 yrs
-
Information about Plain X-ray views are for information only, there are protocols in place within radiography department to ensure appropriate views are performed.
Discussion Points
If time allows, injection of the shoulder provides valuable diagnostic information. Consider using 10mls 0.5% marcain with steroid (e.g. 1ml/40mg of Kenalog) for sub acromial or glenohumeral injection and re-examining after 5-10 minutes: An immediate response is strong supportive evidence for the relevant diagnosis
NHS Shoulder Service Providers in Cornwall
-
- RCHT at various sites
-
Duchy (shoulder and elbow clinic)
-
Duchy Exclusions
-
Significant medical History including major cardiac problems, neurological disabilities,
- Under 18 years
-
Significant medical History including major cardiac problems, neurological disabilities,
-
Duchy Exclusions
References:
Clinical Knowledge Summaries – Shoulder pain
Garg, S et al 2010 Managing rotator cuff disorders www.arthritisresearchuk.org/pdf/TR7.pdf
Mitchell, C 2008 Management of shoulder disorders in primary care www.arthritisresearchuk.org/files/6534_05032010154554
Mitchell, C BMJ 2005;331:1124-8 Shoulder pain: diagnosis and management in primary care
Contributors
Natalie Dawes, General Practitioner & Referral Management Sifter - natalie.dawes@nhs.net
Sean Dixon Consultant Orthopaedic Surgeon, Royal Cornwall Hospital - seandixon@nhs.net
James Wilson Consultant Orthopaedic Surgeon, Royal Cornwall Hospital - james.wilson26@nhs.net
Kim Farmer, Consultant Radiologist, Royal Cornwall Hospital - kim.farmer4@nhs.net
The guidelines above have been developed in conjunction with the RCHT Radiology Department. Should you feel that there is a need for clinical imaging outside of the criteria stated above then you may find it helpful to obtain advice from radiology email enquiries. They aim to respond within 24hrs and the email address is